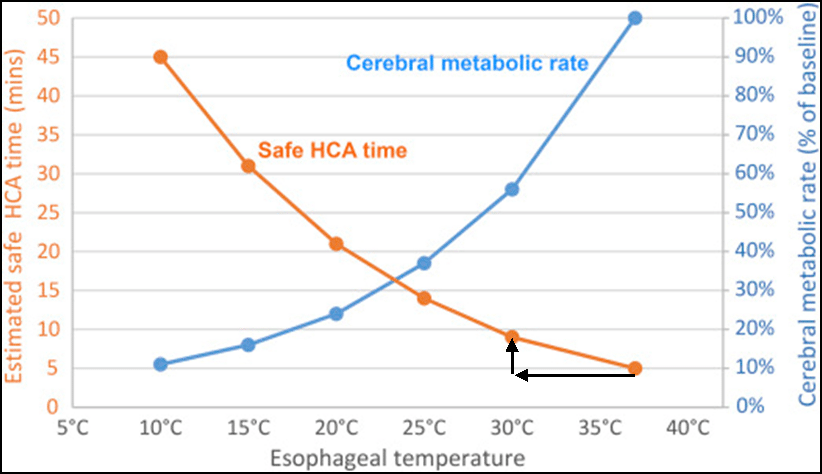
Depressurization incidents during EVA will have hypoxia as the ultimate cause of death or permanent brain damage. If an astronaut’s brain is deprived of oxygen, irreparable damage occurs after about 4 minutes. .. at body temperature. But under conditions of hypothermia (low body temperature), damage occurs much slower.
To illustrate the potential, Hypothermic anesthesia lowers the body temperature to 68-77 °F (20-25 °C) and allows blood flow to the brain to be stopped for up to an hour. https://en.wikipedia.org/wiki/Deep_hypothermic_circulatory_arrest
There is evidence from rescued avalanche suffocation victims that hypothermia is neuro-protective. https://www.resuscitationjournal.com/article/S0300-9572(16)30114-9/pdf#:~:text=Hypothermia%20is%20one%20factor%20in,make%20a%20comparison%20to%20drowning
There are anecdotal cases of downing victims immersed in cold water who have been resuscitated after 30 minutes. The longest time from hypothermic cardiac arrest to return of spontaneous circulation is almost 7 hours. https://www.sciencedirect.com/science/article/pii/S0300957214005243
Back to the astronauts: Most possible fatal events during EVA have cerebral hypoxia as the ultimate cause of death. During EVA depressurization, rescue and successful resuscitation could be enhanced by inducing hypothermia during the emergency retrieval and repressurization.
EVA suits have a Liquid Cooling and Ventilation Garment (LCVG) which has a 2.7 liter water reservoir. It also has a 7000psi emergency supercritical O2 tank. Either of these could be incorporated into an emergency refrigeration device, utilizing latent heat of vaporization.
The lungs have a wetted gas exchange area about the size of a tennis court. While “breathing vacuum”, water would evaporate to try maintain a partial pressure of 47mmHg. This would remove significant heat from pulmonary blood flow and potentially cause rapid core cooling.
Imagine an EVA depressurization, leading to complete loss of pressure. The astronaut would lose consciousness within 15 seconds. The only hope for survival would be re-pressurization. 4 minutes is not very long for the EVA partner to manhandle the unconscious astronaut into an airlock. If an emergency refrigeration device and evaporative pulmonary cooling could lower the body temperature to 30*C during the rescue, this could increase the time to brain death for a few more minutes. Nothing to loose.
This is an unusual proposal, but it is for a very unusual situation. In a hospital, Hypoxia is treated with oxygen and ventilation, which is not available during the EVA rescue. Crash Hypothermia induction using a custom designed total body refrigeration suit is not usually available as an emergency alternative. But this alternative could be available in an EVA suit.
Question: What policies and capabilities are in place to induce hypothermia for the purpose of reducing hypoxic brain damage in EVA astronauts? If not, why not?